Neonatal Monitoring

Most babies in the critical care rooms will be monitored closely. You will see the monitor just above the baby’s cot space. The monitors often display numbers and waveforms in different colours.
Commonly measured parameters are Heart rate, ECG wave forms, Breathing rate, Oxygen levels and Blood pressures. The nurse or the doctors will explain these to you when you first visit the unit.
The monitor will alarm if the parameters are outside the desired range. It is not uncommon for the baby to have measurements outside the desired range for short periods and many of these alarms do not need any specific action apart from being aware of it.
The nurse and doctors are experienced and know if specific actions are required as a result of these alarms and will act accordingly. If you are concerned, please bring this to the attention of the nurse looking after your child and she will explain in more details.
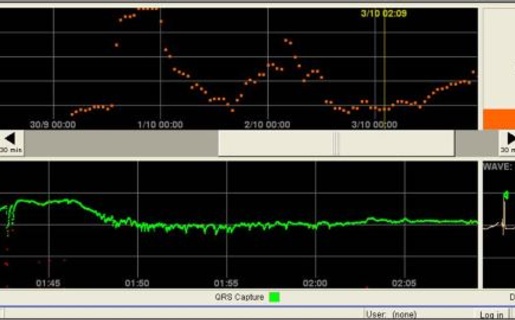
HeRO
Singleton Hospital is the first and one of the very few neonatal units in the UK to have installed one of the most advanced monitoring system for newborns in intensive care that can potentially warn clinicians about an impending deterioration in clinical condition of the baby even before symptoms of illness arise.
The availability of this information to clinicians have been shown in research studies to save lives of very small premature babies in intensive care setting.
You will see this monitoring system displayed in the cot side PCs and the information discussed during ward rounds.
X-rays
Babies undergo different X-ray examinations from time to time during their care on the unit. To avoid unnecessary X-ray exposure, staff may ask you to leave the unit temporarily during the procedure.
Ultrasound
Babies who are born very early or who are very ill often undergo ultrasound scan of their brain to exclude haemorrhage or other abnormalities. If indicated other organs may also be scanned. The scan is very similar to that undertaken on mothers during the pregnancy and is usually well tolerated by the babies and without any side effects. Some of these scans are undertaken as per a routine schedule even when there are no major concerns. You will be informed of the results by a doctor.
Blood spot screening
You will be offered a blood spot screening test for your baby on Day 1 and again within the first week of life.
The purpose of screening is to identify babies who may have rare but serious inherited metabolic conditions such as phenylketonuria, congenital hypothyroidism, sickle cell disorders or cystic fibrosis. Early treatments with medications, special interventions, or changes in diet help to prevent most health problems caused by these conditions. Most babies screened will not have any of these conditions but, for the small number of babies who do, the benefits of screening are enormous. If left untreated, these disorders can lead to illness, physical disability, developmental delay, or death.
Screening your baby for all of these conditions is strongly recommended, but it is not compulsory. If you do not want your baby screened for any or all of these conditions either discuss it with the neonatal nurses in NICU and SCBU. Your decision will be recorded in the hospital records. If you and your baby have been discharged and you do not think your baby has been screened speak with your community midwife or GP.
Blood spot results
Most babies will have normal results, indicating that they are not thought to have any of these conditions. A health professional will usually let parents know the screening results and record it either in their baby's notes or in the baby's personal child health record by the time the child is 6-8 weeks old. If a baby is thought to have one of the conditions, he or she will need further tests to confirm the result. For further information on newborn blood spot screening please ask staff for a leaflet.
Retinopathy of Prematurity (ROP screening)
Children who are born very prematurely may develop eye problems. A common problem is abnormal development of the blood vessels in the retina (at the back of the eye) called retinopathy of prematurity (ROP). Most of these abnormalities resolve on their own, but in a few, the condition may progress rapidly. Laser therapy, if undertaken in a timely manner, can save visual loss. For this reason, every baby born before 32 weeks of pregnancy or who weighed under 1500g at birth, will be examined by an ophthalmologist (hospital eye specialist). At Singleton Hospital, the ophthalmologist will initially see your baby at four to five weeks after delivery and then re-examine your baby's eyes every week or fortnightly, usually on a Wednesday, until it is felt that your baby is no longer at risk. The follow up may continue even after discharge home. In such situations, you will be recalled from home and your baby examined in a special clinic held just outside the neonatal unit. If during admission your baby is transferred back to your booking hospital, the eye examination will be performed locally and the unit will be informed of when it is due.
What is involved in the eye examination?
The eye examination is carried out at the cot-side in the neonatal unit. Your baby is given some eye drops about an hour before the examination which will dilate your baby's pupils to make it easier for the ophthalmologist to see the back of both eyes. The nurse looking after your baby will assist the doctor by holding your baby still while the eye examination is performed. Just before the examination a numbing anaesthetic drop is put in each eye. It is necessary to use a small clip (speculum) to keep the eyelids open and a probe to move the eye into different positions so that the whole retina can be seen.
Premature babies are sensitive to any handling and although the examination may be stressful its importance in preventing blindness means that the eye examination must be carried out. The ophthalmologist is trained to perform the examination quickly with minimal discomfort to your baby. Your baby may cry because he/she is being examined and it is a bit uncomfortable but as soon as the examination is over he/she will settle back to sleep. Following the examination your baby's eyes may be a little red or swollen but this will usually settle within 24 hours.
The ophthalmologist visits the neonatal unit on a weekly basis, usually on a Wednesday. If you have any questions regarding your baby's eyes or vision please ask the nurse or doctors looking after your baby when this visit is due and the ophthalmologist will be pleased to discuss your concerns.
Follow up and further examination
As well as being examined in the NICU, babies who are born very prematurely should also be seen by a hospital eye specialist (Orthoptic or Ophthalmologist) during the first few years to ensure that their vision is developing normally.
Hearing screen
A small number of babies are born with a hearing loss, which is not easy to identify. Screening will allow those babies who have a hearing loss to be identified early. Early identification is known to be important for a child's development. This also means support and information can be provided to the parents at an early stage.
As a national programme, all babies will have their hearing tested before leaving hospital. If your baby's hearing is not screened before you leave hospital, ask your health visitor, midwife or GP to arrange an appointment.
Risk factors for hearing loss
There are some known factors that may put a baby at risk of having a hearing loss, these include:
- Some medical conditions
- Other members of the baby's family have a hearing loss since birth or very early childhood
- Babies that have needed special or intensive care in early infancy
- Premature babies seem to be at a greater risk of having a hearing problem than term babies
How is it done?
The hearing screen uses two simple methods to check the hearing of babies. The test is straightforward, quick, non-invasive and painless.
The screening test will usually be done by a trained hearing screener or your health visitor while your baby is sleeping. You can find out more about your baby's hearing screening from a ward based or community or your health visitor. The newborn hearing screening programme has leaflets available on all of the wards and has a website that provides further information: Link to come
Common procedures
Blood tests
While your baby is in the NICU blood tests will be performed regularly to monitor the body’s organ function and test for signs of infection. The regularity of the blood tests will depend on how sick your baby is. Your baby's blood can be tested on the unit, but some samples will be sent to the laboratory to gain more in depth information. We always use the smallest amount of blood possible and usually take a sample from the heel, an arterial line if your baby already has one or from a fine needle inserted into the vein. The doctors and nurses will be happy to discuss the reasons for the various tests we do and the results as these become available.
Cannulation
Cannulation is the term used for the insertion of a cannula into one of your baby's veins. This cannula is a small plastic tube which allows for the delivery of fluids, medicines and blood transfusions to ensure the well-being of your baby.
Naso/orogastric tube
This is a small feeding tube passed through your baby’s nose or mouth into the stomach. This is primarily used for feeding milk but also used to aspirate excessive fluid or air in the stomach. Once inserted the tube is secured on to your baby’s face with a small adhesive tape and position confirmed using special pH strips that detects acid aspirated from the stomach. The position can also be confirmed on X-rays.
Central lines
In order to give your baby essential nutrients (TPN) and certain drugs, a specialised line needs to be put in which goes into one of the large blood vessels of the body.
These lines are known as central lines or more commonly ‘Long Lines’. To put a long line, a cannula is inserted into one of the veins in the arm, leg or scalp and a tiny tube fed through it which goes all the way to the large blood vessels. Once inserted an x-ray is taken to check the position of the line. The nursing staff will carefully observe these lines for leakage and swelling and will remove them immediately if there are any concerns.
Umbilical lines
The belly button has two of the largest blood vessels in the newborn baby and therefore makes it relatively easy for the doctors to put in a central line. These are usually used in the first few days of life. The venous lines provide access to give nutrition and medication through a drip while the arterial line allows doctors to monitor blood pressure continuously. The arterial line also allows doctors to draw blood without the need to prick the skin every time a blood test is required.
Intubation
If your baby is having problems with breathing and the doctors decide that he/she requires breathing support via a ventilator (breathing machine), an endotracheal tube (ETT) will be inserted into the windpipe through his/her mouth and connected to the ventilator. The part of the tube you can see will be secured to your baby's face to prevent it from moving around while the other end rests in your baby's trachea (windpipe) just above the opening to his/her lungs. Your baby will be given pain relief, sedation and muscle relaxants before placing this tube except in an emergency.
Sepsis screen and lumbar puncture
Infection is a serious illness in a newborn baby. If your baby is showing signs of being unwell or suspected to have an infection, a doctor may decide to perform an infection/ sepsis screen. This is a common procedure on the neonatal unit. To perform a full infection screen the doctor will need to obtain samples of your baby's blood, urine and possibly spinal fluid. These samples will be given to the hospital laboratory to see if they can grow any bacteria, virus or fungi from the samples. Samples may also be taken from your baby's sputum or a swab taken from a wound site. Blood tests including a full blood count (FBC) and C-reactive protein level (CRP) are also taken. These will indicate if the baby is suffering from an infection. In some instances of suspected infection an x-ray of your baby's tummy or chest may be taken.
As part of an infection screen a Lumbar Puncture may be performed to test for meningitis. A Lumbar Puncture is performed by inserting a small hollow needle into the lower part of your baby's spinal canal in between to bones in the lower back to draw out a sample of fluid that surrounds your baby's spinal cord. This is a common procedure and is similar to the epidural or spinal analgesia that you may have received in labour or prior to a Caesarean Section. The fluid collected is called the cerebrospinal fluid (CSF) and it surrounds and protects your baby's brain and spinal cord. Your baby's CSF will then be sent to the laboratory for testing. Analysing the CSF will show if there is a meningitis infection present
The doctors or nurse looking after your baby will try to inform you of the plan to perform an infection screen. However, in an intensive care setting and in particular if you are at home, this is not always possible before the procedure is undertaken. You will be informed of the procedure and results as soon as possible
Antibiotics
These are medicines commonly used to control suspected / proven infection in your baby. Clinicians often have a low threshold of starting antibiotics when they suspect an infection. If the results of the blood tests and subsequent clinical course refute the original suspicion, antibiotics may be stopped quickly. If the infection is proven or strongly suspected, antibiotics may be given for longer periods after discussion with specialist doctors called microbiologists.
Echocardiogram (ECHO)
An echocardiogram is an ultrasound scan of your baby's heart to check the chambers and valves of the heart.
Rydym yn croesawu gohebiaeth a galwadau ffôn yn y Gymraeg neu'r Saesneg. Atebir gohebiaeth Gymraeg yn y Gymraeg, ac ni fydd hyn yn arwain at oedi. Mae’r dudalen hon ar gael yn Gymraeg drwy bwyso’r botwm ar y dde ar frig y dudalen.
We welcome correspondence and telephone calls in Welsh or English. Welsh language correspondence will be replied to in Welsh, and this will not lead to a delay. This page is available in Welsh by clicking ‘Cymraeg’ at the top right of this page.